









Yellow fever is endemic in the WHO African Region and was among the top five most frequently reported events in the region in 2019 and 2020. Twenty-seven countries in Africa have been classified as high-risk by the Eliminate Yellow fever Epidemics (EYE) global strategy. From 1 January 2021 to 26 August 2022, a total of 12 countries in the region have reported 184 confirmed cases and 274 probable cases, including 21 deaths, reflecting ongoing complex viral transmission.
Risk factors for onward spread and amplification include low population immunity, population movements, viral transmission dynamics, and climate and ecological factors that have contributed to the spread of Aedes mosquitoes. Response measures, most notably reactive and preventive vaccination campaigns, are ongoing in the affected countries. Since the beginning of 2021, over 3.9 million people have been vaccinated through reactive vaccination campaigns in Cameroon, Central African Republic, Chad, Ghana, and Kenya.
Description of outbreaks
In 2021, nine African countries – Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of Congo, Gabon, Ghana, Nigeria, and Republic of the Congo – reported a total of 151 confirmed cases of yellow fever (for more details, please see the Disease Outbreak News published on 23 December 20211). Of these nine countries, six continue to report confirmed cases of yellow fever with ongoing transmission in 2022, while Côte d’Ivoire and Nigeria have reported probable cases2 and Gabon has not reported further cases since 2021.
In 2022, two additional countries, Kenya3 and Uganda4, have reported confirmed cases of yellow fever. From 1 January to 26 August 2022, a total of 33 confirmed cases of yellow fever were reported from eight African countries including Central African Republic (33%, 11 cases), Cameroon (24%, eight cases), Democratic Republic of Congo (13%, four cases), Kenya (9%, three cases), Chad (6%, two cases), Republic of the Congo (6%, two cases), Uganda (6%, two cases), and Ghana (3%, one case).
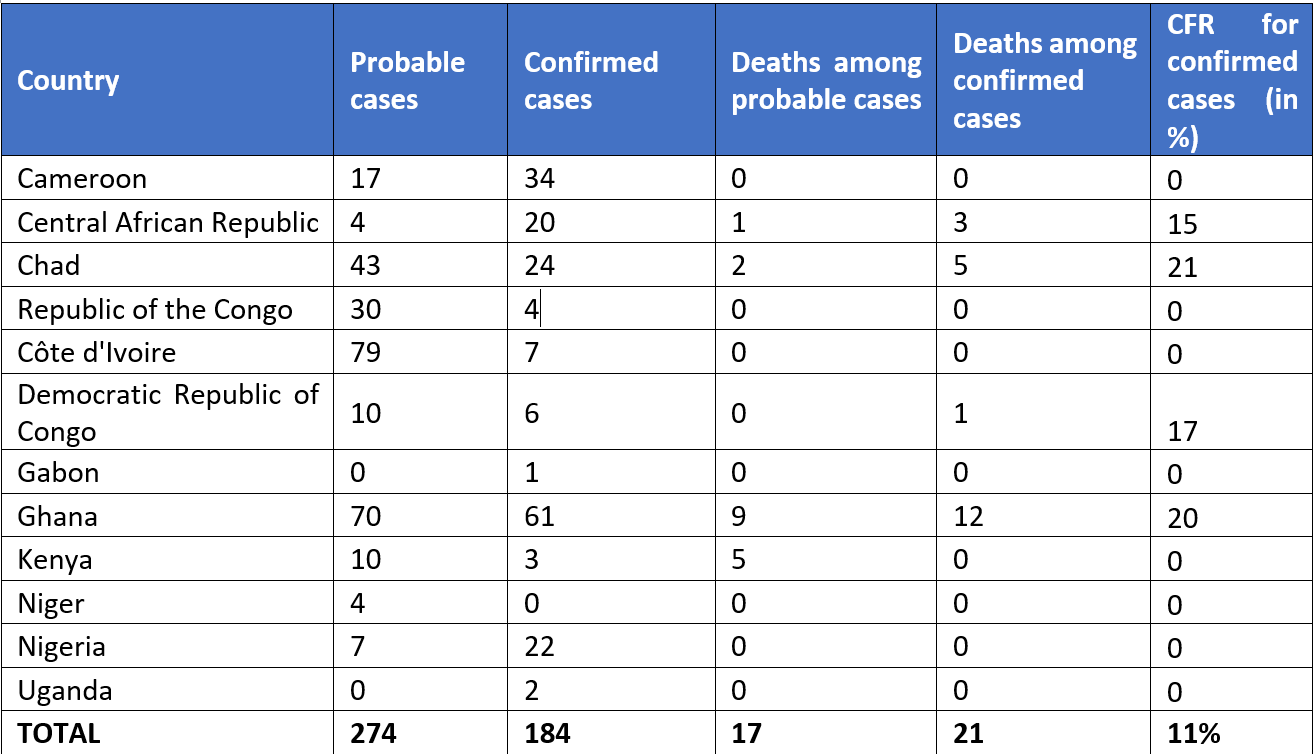
Ten countries – Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of Congo, Ghana, Kenya, Niger, Nigeria, and Republic of the Congo – have also reported a total of 274 probable cases of yellow fever from 1 January 2021 to 26 August 2022 (Table 1).
The majority of cases over the entire period were reported in the last quarter of 2021 (Figure 1), with Ghana reporting around 33% of all confirmed cases. Of 184 confirmed cases, 73% are aged 30 years and below, and the male-to-female ratio is 1.2. The case count and the number of outbreaks are anticipated to continue evolving as the Region enters the seasonal period when there is often an increase in cases notified.
Figure 1. Probable and confirmed cases of yellow fever by week of symptom onset in countries reporting transmission in the WHO African Region, 1 January 2021 to 26 August 2022.

Figure 2. Distribution of probable and confirmed cases of yellow fever in the WHO African Region, 1 January 2021 to 26 August 2022.

Table 1. Probable and confirmed cases of yellow fever and deaths by country in the WHO African Region, 1 January 2021 to 26 August 2022.
Epidemiology of yellow fever
Yellow fever is an epidemic-prone, vaccine-preventable disease caused by an arbovirus transmitted to humans by the bites of infected Aedes and Haemagogus mosquitoes. The incubation period ranges from 3 to 6 days. Many people do not experience symptoms, but when they occur the most common are fever, muscle pain with prominent backache, headache, loss of appetite, and nausea or vomiting. In most cases, symptoms clear after 3 to 4 days. A small proportion of cases progress to the toxic phase with systemic infection affecting the liver and kidneys. These individuals can have more severe symptoms of high-grade fever, abdominal pain with vomiting, jaundice and dark urine caused by acute liver and kidney failure. Bleeding can occur from the mouth, nose, eyes, or stomach. Death can occur within 7 – 10 days in about half of cases with severe symptoms.
Yellow fever is prevented by an effective vaccine, which is safe and affordable. A single dose of yellow fever vaccine is sufficient to grant sustained immunity and life-long protection against yellow fever disease. A booster dose of the vaccine is not needed. The vaccine provides effective immunity within 10 days for 80-100% of people vaccinated, and within 30 days for more than 99% of people vaccinated.
According to the EYE strategy, twenty-seven countries in the African region are high-risk countries for yellow fever based on timing and intensity of yellow fever virus transmission, transmission potential and assessment of urban risk. Re-emergence of yellow fever was reported in 2020 with two outbreaks in West African countries with history of mass vaccination (in Guinea and Senegal, now contained). Since late 2021, the situation has intensified with 12 countries across the region reporting probable and confirmed cases.
WHO assesses the risk at regional level to be high. Current multi-country outbreaks and active virus circulation in West, Central and East Africa have resulted in increased morbidity and mortality, with continued risk of amplification and spread. The immunization coverage for yellow fever has been suboptimal in most of the affected countries and in specific populations. According to WHO and UNICEF estimates, in 2021, the routine childhood vaccination immunization coverage for yellow fever in the African region was 47%. This is much lower than the 80% threshold required to confer population immunity against yellow fever, indicating that a large population remains susceptible to yellow fever with a risk of continued transmission.
Immunization coverage by countries reporting probable and confirmed cases in West, Central and East Africa are as follows: Cameroon (54%), Central African Republic (41%), Chad (45%), Republic of the Congo (67%), Côte d’Ivoire (65%), Democratic Republic of the Congo (56%), Gabon (53%), Ghana (94%), Kenya (7%), Niger (80%), and Nigeria (63%). Uganda plans to introduce yellow fever vaccine into routine immunization in August 2022. Further information on immunization coverage can be found here.
Many countries in West, Central, and East Africa have been facing political instability and insecurity, in addition to concurrent outbreaks (including COVID-19, Ebola virus disease, cholera, meningitis, malaria, monkeypox, circulating vaccine-derived poliovirus type 2 (cVDPV2), chikungunya, leishmaniasis, plague, Lassa fever, etc.). These could contribute to delayed case investigation and hinder the surveillance and response efforts against yellow fever.
The risk at global level is assessed to be low as no exported cases of yellow fever linked to these 12 countries with probable or confirmed cases since January 2021 have been reported.








{kind=link}
Discussion about this post